

Obesity Management as a Primary Treatment Goal for Type 2 Diabetes – It’s Time for a Paradigm Shift
Obesity has been established as one of the key risk factors for type 2 diabetes. This has led to growing interest in obesity management to supplement glycemic management as a treatment goal for type 2 diabetes.
Ricardo Cohen, a surgeon from the Oswaldo Cruz German Hospital, and Ivania Rizo, an endocrinologist from Boston Medical Center, presented current therapeutic options for obesity management at the American Diabetes Association 82nd annual Scientific Sessions.
As a surgeon, Cruz strongly supports bariatric surgery. He presented the results of a study showing that 73% of participants who had a form of bariatric surgery reduced their hypertension (high blood pressure) medications by 30% while maintaining a blood pressure of less than 140/90 mmHg. He followed this with results from another study that showed there was al 41% decrease in mortality for participants who had bariatric surgery versus those who did not have the surgery.
When looking specifically at the participants who had pre-existing type 2 diabetes, there was an even greater (around 60%) reduction in mortality. He supported this information with safety data that shows only a 3.4% composite complications rate for people undergoing a type of bariatric surgery called RYGB.
In a meta analysis of all the current studies investigating type 2 diabetes remission after baritric surgery, there was a 72% remission rate for people with BMIs under 35 and a 71% remission rate for people with BMIs over 35.
Overall, bariatric surgery leads to long term significant weight loss, type 2 diabetes remission, improved kidney health, and a decrease in heart disease risk factors. He concluded by suggesting that lifestyle changes should be tried first, and then medications should be provided to combat obesity. If the person does not respond well to either, then surgery is a good option and it might be ideal if the person took anti-obesity medications after the surgery for a combination therapy.
Rizo followed up with a presentation on the treatment of both diabetes and obesity. In the figure below, she overviewed the efficacy of current anti-obesity drugs. She highlighted that the addition of Semaglutide (a GLP-1 receptor agonist) and Tirzepatide have revolutionized obesity management with their impressive weight reduction results. However, it should be noted that tirzepatide is not yet approved in the US by the FDA for the treatment of weight loss, specifically.
She went into detail how researchers currently believe Tirzepatide works in the body as a dual GIP and GLP-1 receptor agonist. Tirzepatide is attracted to, and binds with, the same GIP receptors in your cells as the GIP hormone that your body naturally makes. Additionally it is also attracted to, and binds with, the same GLP-1 receptors in your cells as your body’s natural GLP-1 hormone, however, this connection is about five times weaker (than the natural hormone). GLP-1 is the main hormone in your that results in a decrease in blood sugar and reduces appetite.
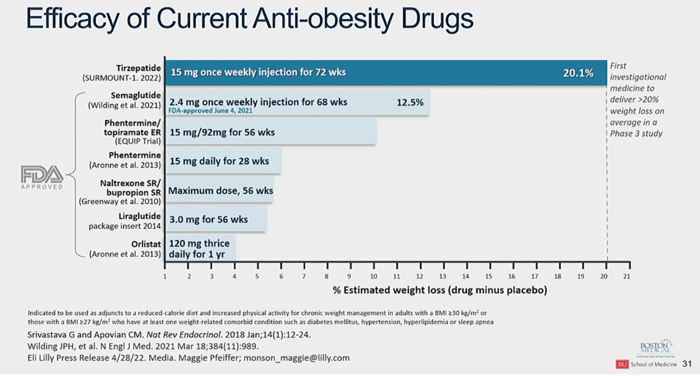
This chart compares the average estimated percent weight loss for tirzepatide along with current FDA-approved weight-loss medications. Tirzepatide far surpasses the weight loss results shown by currently available medications.
From www.diatribe.org
Nyhetsinfo
www red DiabetologNytt